|
|
|
The following promotional message is brought to you by Amgen.
For the treatment of postmenopausal women with osteoporosis at high risk for fracture.
Learn more about a head-to-head bone mineral density (BMD) study evaluating patients continuing on alendronate or transitioning to Prolia® (denosumab)
|
|
|
|
INDICATION
Prolia® is indicated for the treatment of postmenopausal women with osteoporosis at high risk for fracture, defined as a history of osteoporotic fracture, or multiple risk factors for fracture; or patients who have failed or are intolerant to other available osteoporosis therapy. In postmenopausal women with osteoporosis, Prolia® reduces the incidence of vertebral, nonvertebral, and hip fractures.
|
|
|
|
CONTRADICTIONS
Prolia® is contraindicated in patients with hypocalcemia, women who are pregnant, and patients with a history of systemic hypersensitivity to any component of the product. Perform pregnancy testing in women of reproductive potential prior to initiating treatment with Prolia®.
Please scroll below for additional Important Safety Information.
|
|
|
|
Dear [Insert Customer Name],
|
|
|
FREEDOM: Pivotal Phase 3 Fracture Trial
PIVOTAL PHASE 3 FRACTURE TRIAL STUDY DESIGN1,2
A multicenter, international, randomized, double-blind, placebo-controlled clinical trial that studied postmenopausal women between 60 and 90 years of age with a BMD T-score between -2.5 and 4.0 at the lumbar spine or total hip.
7808 patients were randomized to receive Prolia® 60 mg (n = 3902) or placebo (n = 3906) subcutaneously every 6 months. All patients were supplemented with daily calcium and vitamin D.
PRIMARY END POINT1,2
SECONDARY END POINTS1,2
*Composite measurement excluding pathological fractures and those associated with severe trauma, fractures of the vertebrae,
skull, face, mandible, metacarpals, fingers, and toes.
|
RESULTS OF THE PIVOTAL PHASE 3 FRACTURE TRIAL1-3
During the pivotal Phase 3 fracture trial in postmenopausal women with osteoporosis, Prolia® significantly reduced the relative risk of fracture at 3 years in vertebral (68%†), hip (40%‡), and nonvertebral (20%§) sites (vs placebo).
There were no significant differences between subjects who received denosumab and those who received placebo in the total incidence of adverse events, serious adverse events, or discontinuation of study treatment because of adverse events.
Adverse reactions most commonly reported (≥ 5% and more common than placebo) in the Prolia®-treated group were back pain (34.7%), pain in extremity (11.7%), musculoskeletal pain (7.6%), hypercholesterolemia (7.2%), and cystitis (5.9%).
†Absolute risk reduction: 4.8% (P < 0.0001).
‡Absolute risk reduction: 0.3% (P = 0.04).
§Absolute risk reduction: 1.5% (P = 0.01).
|
|
|
|
|
STAND: Prolia® vs Alendronate
In a 1-year, multicenter, international, randomized, double-blind, double-dummy, parallel-group phase 3 trial4
The primary endpoint was the percent change in total hip BMD from baseline to month 12, and select secondary endpoints focused on percent change at lumbar spine BMD at 12 months.4
Statistical Analysis4
A step-down multiple testing procedure was used
1. If noninferiority of denosumab for total hip BMD at month 12 was demonstrated by a lower bound of the 95% CI to be greater than -0.35%, then;
2. superiority for the percent reduction in CTX-I at month 3 would be tested, and if the p value was > 0.05, superiority would be stated, and;
3. superiority of total hip BMD at month 12 would be tested; if the p value was > 0.05, then superiority would be demonstrated, and;
4. noninferiority at the lumbar spine would be tested and demonstrated if the lower bound of the 95% CI was greater than -0.22%
Key Inclusion Criteria4
Postmenopausal women age 55 years and older with a BMD T-score of ≤ -2.0 and ≥ -4.0 at the lumbar
spine or total hip Patients must have been receiving alendronate 70 mg/week for ≥ 6 months prior to screening
PROLIA® DEMONSTRATED NONINFERIORITY AND SUPERIORITY
(VS ALENDRONATE) IN TOTAL HIP BMD4,**
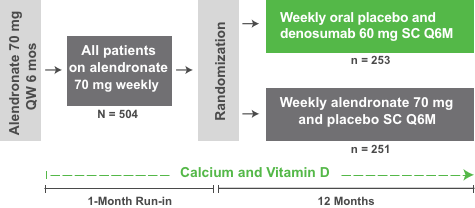
Q6M=once every 6 months; QW=once a week; SC=subcutaneous.
PATIENTS CONTINUING ON ALENDRONATE THERAPY OR TRANSITIONING TO PROLIA® WERE EVALUATED4
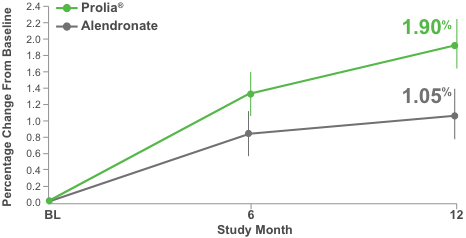
The lower limit of the confidence interval excluded the prespecified noninferiority margin (-0.35% for total hip), thus showing the noninferiority of Prolia® compared with alendronate. Superiority testing demonstrated that the BMD increase with denosumab at the total hip was statistically superior to the change with alendronate (P < 0.0001).
**Primary efficacy endpoint.
††95% CI 0.44%-1.25%, P < 0.01.
BMD data results are not meant to imply fracture efficacy and should not be extrapolated to predict differences in fracture efficacy. Head-to-head fracture studies have not been conducted.
PROLIA® DEMONSTRATED NONINFERIORITY (VS ALENDRONATE)
AND SHOWED STATISTICALLY ISGNIFICANT CHANGES IN LUMBAR SPINE BMD4,‡‡
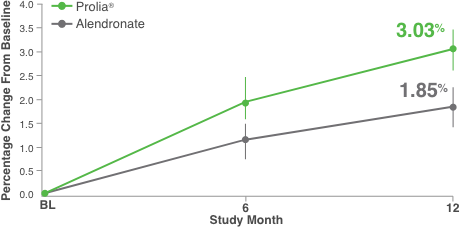
The lower limit of the confidence interval excluded the prespecified noninferiority margin (-0.22% for lumbar spine), thus showing the noninferiority of Prolia® compared with alendronate.
‡‡Secondary endpoint.
§§95% CI 0.63%-1.73%, P < 0.01.
BMD data results are not meant to imply fracture efficacy and should not be extrapolated to predict differences in fracture efficacy. Head-to-head fracture studies have not been conducted.
A SIMILAR NUMBER OF STUDY PARTICIPANTS IN EACH TREATMENT GROUP REPORTED ADVERSE EVENTS DURING THE STUDY (78% PROLIA®, 79% ALENDRONATE)4
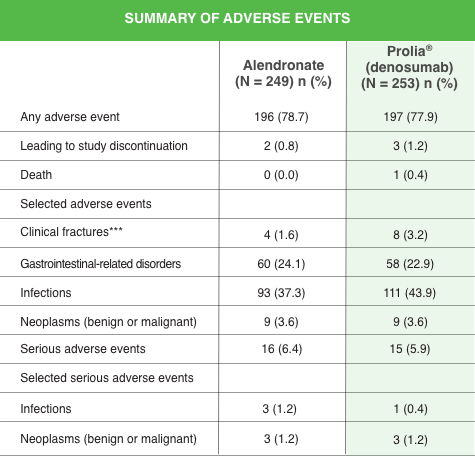
The most frequent adverse events in the Prolia® and alendronate groups, respectively, were nasopharyngitis (13.4% and 10.8%), back pain (10.7% and 11.6%), bronchitis (6.3% and 5.6%), arthralgia (5.9% and 10.4%), constipation (5.1% and 4.8%), and pain in an extremity (4.7% and 8.4%).
***On-study clinical fractures were as follows: Prolia®–2 foot, 2 wrist, 1 radius, 1 fibula, 1 humerus, 1 pelvis, 1 rib, 1 tibia; alendronate–1 foot, 1 wrist, 1 radius, 1 sacrum.
|
|
|
Help lead your members to stronger bones with access to Prolia®.1,4
Please visit proliapayerresources.com for more information
|
|
|
IMPORTANT SAFETY INFORMATION
Contraindications: Prolia® is contraindicated in patients with hypocalcemia. Pre-existing hypocalcemia must be corrected prior to initiating Prolia®. Prolia® is contraindicated in women who are pregnant and may cause fetal harm. In women of reproductive potential, pregnancy testing should be performed prior to initiating treatment with Prolia®. Prolia® is contraindicated in patients with a history of systemic hypersensitivity to any component of the product. Reactions have included anaphylaxis, facial swelling and urticaria.
Same Active Ingredient: Prolia® contains the same active ingredient (denosumab) found in XGEVA®. Patients receiving Prolia® should not receive XGEVA®.
Hypersensitivity: Clinically significant hypersensitivity including anaphylaxis has been reported with Prolia®. Symptoms have included hypotension, dyspnea, throat tightness, facial and upper airway edema, pruritus and urticaria. If an anaphylactic or other clinically significant allergic reaction occurs, initiate appropriate therapy and discontinue further use of Prolia®.
Hypocalcemia: Hypocalcemia may worsen with the use of Prolia®, especially in patients with severe renal impairment. In patients predisposed to hypocalcemia and disturbances of mineral metabolism, including treatment with other calcium-lowering drugs, clinical monitoring of calcium and mineral levels is highly recommended within 14 days of Prolia® injection. Concomitant use of calcimimetic drugs may worsen hypocalcemia risk and serum calcium should be closely monitored. Adequately supplement all patients with calcium and vitamin D.
Osteonecrosis of the Jaw (ONJ): ONJ, which can occur spontaneously, is generally associated with tooth extraction and/or local infection with delayed healing, and has been reported in patients receiving Prolia®. An oral exam should be performed by the prescriber prior to initiation of Prolia®. A dental examination with appropriate preventive dentistry is recommended prior to treatment in patients with risk factors for ONJ such as invasive dental procedures, diagnosis of cancer, concomitant therapies (e.g. chemotherapy, corticosteroids, angiogenesis inhibitors), poor oral hygiene, and co-morbid disorders. Good oral hygiene practices should be maintained during treatment with Prolia®. The risk of ONJ may increase with duration of exposure to Prolia®.
For patients requiring invasive dental procedures, clinical judgment should guide the management plan of each patient. Patients who are suspected of having or who develop ONJ should receive care by a dentist or an oral surgeon. Extensive dental surgery to treat ONJ may exacerbate the condition. Discontinuation of Prolia® should be considered based on individual benefit-risk assessment.
Atypical Femoral Fractures: Atypical low-energy, or low trauma fractures of the shaft have been reported in patients receiving Prolia®. Causality has not been established as these fractures also occur in osteoporotic patients who have not been treated with antiresorptive agents.
During Prolia® treatment, patients should be advised to report new or unusual thigh, hip, or groin pain. Any patient who presents with thigh or groin pain should be evaluated to rule out an incomplete femur fracture. Interruption of Prolia® therapy should be considered, pending a risk/benefit assessment, on an individual basis.
Multiple Vertebral Fractures (MVF) Following Discontinuation of Prolia® Treatment:
Following discontinuation of Prolia® treatment, fracture risk increases, including the risk of multiple vertebral fractures. New vertebral fractures occurred as early as 7 months (on average 19 months) after the last dose of Prolia®. Prior vertebral fracture was a predictor of multiple vertebral fractures after Prolia® discontinuation. Evaluate an individual’s benefit/risk before initiating treatment with Prolia®. If Prolia® treatment is discontinued, patients should be transitioned to an alternative antiresorptive therapy.
Serious Infections:
In a clinical trial (N = 7808), serious infections leading to hospitalization were reported more frequently in the Prolia® group than in the placebo group. Serious skin infections, as well as infections of the abdomen, urinary tract and ear, were more frequent in patients treated with Prolia®.
Endocarditis was also reported more frequently in Prolia®-treated patients. The incidence of opportunistic infections and the overall incidence of infections were similar between the treatment groups. Advise patients to seek prompt medical attention if they develop signs or symptoms of severe infection, including cellulitis.
Patients on concomitant immunosuppressant agents or with impaired immune systems may be at increased risk for serious infections. In patients who develop serious infections while on Prolia®, prescribers should assess the need for continued Prolia® therapy.
Dermatologic Adverse Reactions: Epidermal and dermal adverse events such as dermatitis, eczema and rashes occurred at a significantly higher rate with Prolia® compared to placebo. Most of these events were not specific to the injection site. Consider discontinuing Prolia® if severe symptoms develop.
Musculoskeletal Pain: Severe and occasionally incapacitating bone, joint, and/or muscle pain has been reported in patients taking Prolia®. Consider discontinuing use if severe symptoms develop.
Suppression of Bone Turnover: Prolia® resulted in significant suppression of bone remodeling as evidenced by markers of bone turnover and bone histomorphometry. The significance of these findings and the effect of long-term treatment are unknown. Monitor patients for consequences, including ONJ, atypical fractures, and delayed fracture healing.
Adverse Reactions: The most common adverse reactions (>5% and more common than placebo) are back pain, pain in extremity, musculoskeletal pain, hypercholesterolemia, and cystitis. Pancreatitis has been reported with Prolia®.
The overall incidence of new malignancies was 4.3% in the placebo group and 4.8% in the Prolia® group. A causal relationship to drug exposure has not been established. Denosumab is a human monoclonal antibody. As with all therapeutic proteins, there is potential for immunogenicity.
References: 1. Prolia® (denosumab) prescribing information, Amgen. 2. Cummings SR, San Martin J, McClung MR, Siris ES, Eastell R, Reid IR, et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N Engl J Med. 2009;361:756-765. 3. Bone HG, Wagman RB, Brandi ML, Brown JP, Chapurlat R, Cummings SR, et al. 10 years of denosumab treatment in postmenopausal women with osteoporosis: results from the phase 3 randomized FREEDOM trial and open-label extension. Lancet Diabetes Endocrinol. 2017;5:513-523. 4. Kendler DL, Roux C, Benhamou CL, Brown JP, Lillestol M, Siddhanti S, et al. Effects of denosumab on bone mineral density and bone turnover in postmenopausal women transitioning from alendronate therapy. J Bone Miner Res. 2010;25:72-81.
|
|
|
Amgen Inc.
One Amgen Center Drive
Thousand Oaks, CA 91320-1799
www.amgen.com
© 2020 Amgen Inc. All rights reserved.
USA-162-82584 12/20
|
|
|
|
|
|
|
